
there is a paper somewhere which I cannot find off hand which I have seen a few years ago.
the percent of smallLDL to LDL-P# and being below 10% has reduced risk.
so in a way both views have merit but still LDL-P# must be in the normal range for one to be in a lower risk category.
Rhonda Patrick interviews Peter Attia
-
GenePoole0304
- Contributor

- Posts: 561
- Joined: Mon Nov 10, 2014 7:20 pm


Re: Rhonda Patrick interviews Peter Attia
Gene, I'd love to see that paper if you can find it.
LG1, that's very kind of you. Yes, I did see that Dr. Patrick has an ApoE4 paper in the works. She mentioned that in this podcast taped in Fall of 2015. I bet she's made some decent progress by now. Let me check with Thumperama/Chris to see if he's already reached out. Otherwise, I will. We hate to overwhelm her or maybe a blitz would work . We would love for her to join the site and post in our Guest Researcher & Clinician discussion category. It would be awesome if she could take a few questions like Dr. Dayspring did. With a pending paper, she may not want to spill the beans, but it doesn't hurt for us to ask...
. We would love for her to join the site and post in our Guest Researcher & Clinician discussion category. It would be awesome if she could take a few questions like Dr. Dayspring did. With a pending paper, she may not want to spill the beans, but it doesn't hurt for us to ask...
LG1, that's very kind of you. Yes, I did see that Dr. Patrick has an ApoE4 paper in the works. She mentioned that in this podcast taped in Fall of 2015. I bet she's made some decent progress by now. Let me check with Thumperama/Chris to see if he's already reached out. Otherwise, I will. We hate to overwhelm her or maybe a blitz would work
-
thumperama

- Senior Contributor

- Posts: 173
- Joined: Mon Aug 11, 2014 11:54 am
Re: Rhonda Patrick interviews Peter Attia
Julie & LG,
I did just that earlier today.
Dr Attia replied to my request and said if we have Dayspring & Patrick, he didn't believe he would have much to add. So, I contacted her via her site.
I did just that earlier today.
Dr Attia replied to my request and said if we have Dayspring & Patrick, he didn't believe he would have much to add. So, I contacted her via her site.
Re: Rhonda Patrick interviews Peter Attia
I'm personally more interested in waiting patiently for her paper, to see her thoughts explicated comprehensively and systematically. That's not to say I wouldn't jump to see what she might offer our forum before that!
ApoE 3/4 > Thanks in advance for any responses made to my posts.

Re: Rhonda Patrick interviews Peter Attia
thumperama wrote:Julie & LG,
I did just that earlier today.
Dr Attia replied to my request and said if we have Dayspring & Patrick, he didn't believe he would have much to add. So, I contacted her via her site.
no no no - can we have Attia as well? He is AWESOME.
Can we beg him?
Re: Rhonda Patrick interviews Peter Attia
Thanks for reaching out to both, Chris!

Re: Rhonda Patrick interviews Peter Attia
Finally got a chance to listen to this.
Reinforced Gundry's focus on a) minimizing inflammation (as did Bredesen's talk), b) limiting animal protein intake to 20g/day so as to not spike IGF-1 (methionine) and activate mTOR (leucine), c) explained that my high sex binding hormone globulin is expected with this diet which means my free testosterone can be low (Dr. Gundry has me supplement with DHEA to increase testosterone and offset this).
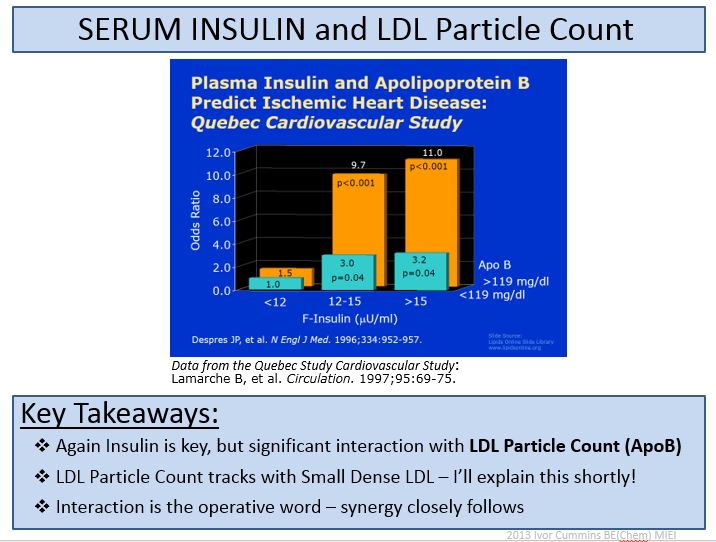
As to Apo B/LDL-P, engineer Ivor Cummins has relooked at some of the data that actually contain insulin. In many cases the Apo B signal with respect to heart disease is very muted when insulin is low and exaggerated when insulin is high. As I recall, Julie posted something for E4's, perhaps in Nov 2014, that showed this, too.
Here is one of his slides: http://www.thefatemperor.com/blog/2015/ ... roscleosis
ApoB/ApoA-1 appears to be a better metric (previously posted by Julie somewhere):
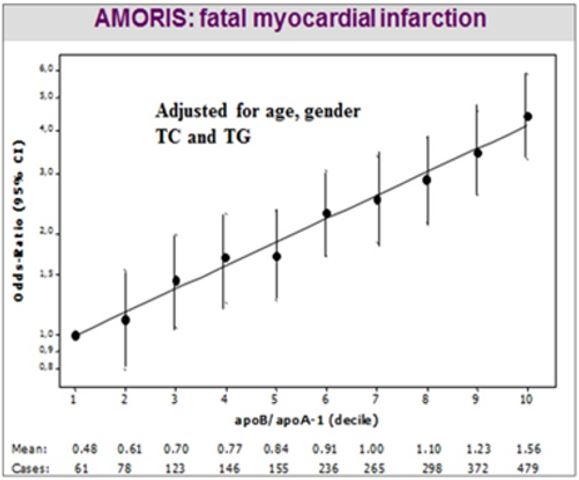
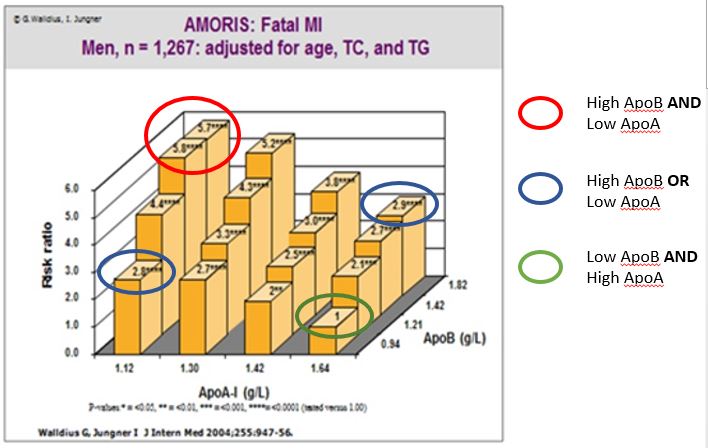
http://www.thefatemperor.com/blog/2016/ ... e-is-apoa1
When Cummins Tweeted the graph here
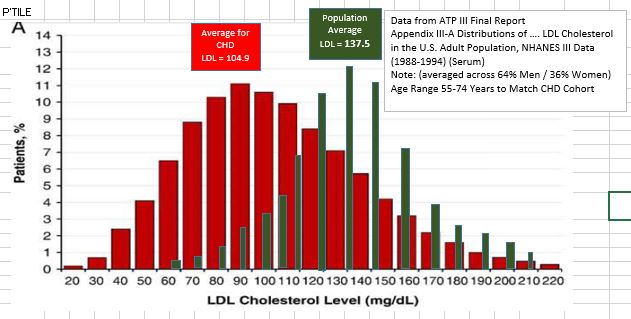
to Dr. Dayspring, Dayspring replied, "Current NHANES data: majority of MI are explained by IR. But real message is unless >200 mg/dL - LDLc is terrible biomarker. " http://www.thefatemperor.com/blog/2014/ ... ic-foolery
Based on Kraft's work http://www.thefatemperor.com/blog/2015/ ... -missed-it, I'm guessing all the LDL-type data are corrupted with most of the population having an abnormal insulin response. As Kraft said "diabetes in-situ." For those who have not read his book, the punch line from 14,000+ 5 hour oral glucose tolerance tests with insulin assay is that only 20% of those with a normal glucose response had a normal insulin response - then there were all the rest who had an abnormal insulin response (You need to be at 3-5 μU/ml fasting insulin to be completely in the clear without the full assay). Cummings makes a good case for this in some of these posts: http://www.thefatemperor.com/blog/2016/ ... hvmhds1sa3
Reinforced Gundry's focus on a) minimizing inflammation (as did Bredesen's talk), b) limiting animal protein intake to 20g/day so as to not spike IGF-1 (methionine) and activate mTOR (leucine), c) explained that my high sex binding hormone globulin is expected with this diet which means my free testosterone can be low (Dr. Gundry has me supplement with DHEA to increase testosterone and offset this).
As to Apo B/LDL-P, engineer Ivor Cummins has relooked at some of the data that actually contain insulin. In many cases the Apo B signal with respect to heart disease is very muted when insulin is low and exaggerated when insulin is high. As I recall, Julie posted something for E4's, perhaps in Nov 2014, that showed this, too.
Here is one of his slides: http://www.thefatemperor.com/blog/2015/ ... roscleosis
ApoB/ApoA-1 appears to be a better metric (previously posted by Julie somewhere):
http://www.thefatemperor.com/blog/2016/ ... e-is-apoa1
When Cummins Tweeted the graph here
to Dr. Dayspring, Dayspring replied, "Current NHANES data: majority of MI are explained by IR. But real message is unless >200 mg/dL - LDLc is terrible biomarker. " http://www.thefatemperor.com/blog/2014/ ... ic-foolery
Based on Kraft's work http://www.thefatemperor.com/blog/2015/ ... -missed-it, I'm guessing all the LDL-type data are corrupted with most of the population having an abnormal insulin response. As Kraft said "diabetes in-situ." For those who have not read his book, the punch line from 14,000+ 5 hour oral glucose tolerance tests with insulin assay is that only 20% of those with a normal glucose response had a normal insulin response - then there were all the rest who had an abnormal insulin response (You need to be at 3-5 μU/ml fasting insulin to be completely in the clear without the full assay). Cummings makes a good case for this in some of these posts: http://www.thefatemperor.com/blog/2016/ ... hvmhds1sa3
Tincup
E3,E4
E3,E4
